


This article covers diagnosing and treating urinary incontinence in dogs, which involves involuntary urine leakage. It covers the distinction between incontinence, increased urine output (polyuria), and frequent urination (pollakiuria), and lists common signs like bed-wetting and dribbling. The article also previews medical and surgical treatment options available for managing this condition.
Incontinence is defined as involuntary urine leakage during the storage phase of micturition, when the bladder should be filling with urine. Usually, the voiding phase is initiated when intravesical pressure reaches 50 cmH2O. However, in patients suffering from urinary incontinence, micturition occurs before that.
Urinary incontinence, polyuria, pollakiuria: what is the difference?
Definitions:
- Urinary incontinence: involuntary urine leakage
- Polyuria: increased amount of urine output
- Pollakiuria: increased frequency of urination, normally with small volumes of urine each time
Dogs with urinary incontinence usually present with:
- History of wetting the bed while sleeping
- History of dribbling urine around the house
- History of leaving a small wet patch of urine where they lay
- Stained prepuce, abdominal, perivulvar area or pelvic limbs
- Recurrent urinary tract infections
If the owner is not able to describe the clinical signs well, ask them to provide a video. Some dogs may present as being “incontinent” when in reality they might be suffering from polyuria or pollakiuria.
Differential diagnosis of urinary incontinence in dogs
Overflow incontinence: the most common reason for overflow is chronic urinary retention, particularly if due to poor detrusor muscle contractility (urinary bladder atony) secondary to neurological (LMN injuries to S1-S3, pelvic or pudendal nerve, UMN above sacrum affecting spinal cord or brainstem micturition centre) and non-neurological (overdistension) conditionsPrimary bladder disease/Poor bladder storage:
-
- Hypercontractility due to:
- Urinary tract infection
- Inflammation
- Infiltrative neoplasm
- Partial urethral obstruction
- Urinary bladder hypoplasia: very small bladder such that it cannot contain normal volumes of urine
- Detrusor muscle instability: involuntary contractions of the detrusor muscle
- Hypercontractility due to:
-
-
- Ectopic ureters: ureters may terminate in urethra, vagina and even in the uterus and can be intramural or extramural
- Patent urachus: condition in which there is a complete or remnant structure connecting the urinary bladder and the umbilicus. Recurrent urinary tract infections are common in these cases.
- Urethro-vaginal fistula: anatomical connection between the urethra and the vagina
- Vaginal vestibular stenosis: urine accumulates in the vaginal vestibule and leaks when, for example, they sit down.
- Intrapelvic bladder: the bladder neck is particularly short and therefore when the urinary bladder is full, the pelvic canal increases the intravesical pressure.
- Urethrorectal fistula: continuous dribbling urine from rectum (rare)
-
Diagnostic pathway for urinary incontinence
- Detailed history to ensure accurate information on the issue is obtained (see owner questionnaire below)
- Observe the pet urinating, and assess for leakage when moving around or lying down
- Palpate bladder and note size, tone and whether manual expression is possible (normally not easy).
- Repeat palpation after voiding to assess completeness of emptying.
- Evaluate external genitalia, perineum, perform vaginal examination and rectal examination.
- Assess neurological function.
- Perform urinalysis, ideally from a cystocentesis urine sample
- Chemical analysis: If SG low investigate for polyuria and polydipsia (PU/PD)
- Urinary sediment: if there is an inflammatory sediment, perform culture
- Urine cytology: if neoplasia is a consideration, this can be more sensitive than sediment alone
- Haematology & biochemistry analysis to exclude systemic conditions, including CKD and causes of PU/PD
- Pass urine catheter to assess patency (NB not foolproof - some obstructions may be small and missed with this) and measure urine residual volume (normal 0.2-0.4 mL/kg)
- Imaging:
- Survey abdominal radiographs
- Assess position of the urinary bladder (intrapelvic urinary bladder, bladder in perineal hernia), size of prostate, presence of radiodense uroliths
- Ultrasound examination of the bladder, bladder trigone and prostate gland. Assessment of other areas of the urogenital tract can also be helpful.
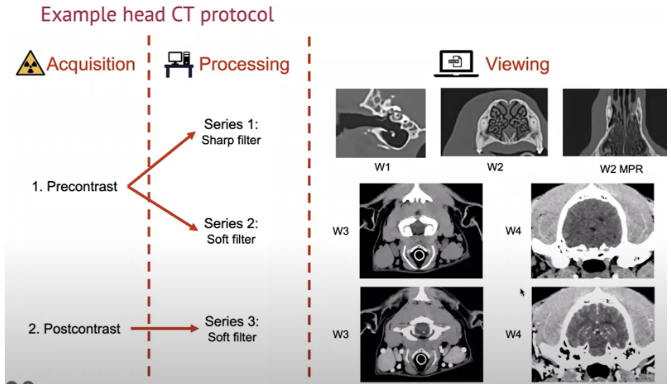
- Excretory intravenous urogram - ideally CT or fluoroscopy
- Evaluates the urine flow from the kidneys to the urinary bladder – great for detecting the presence of ectopic ureters
- Contrast radiographs might be able to identify ectopic ureters but fluoroscopy or contrast CT are more sensitive imaging modalities
- Retrograde vagino-urethrogram (females) and retrograde urethrogram (males) - contrast radiography, contrast CT or fluoroscopy
- Evaluate the lower urinary tract and vagina (females) while being filled with radiopaque contrast medium, and may be needed to identify ectopic ureters entering distally
- Survey abdominal radiographs
- Urethrocystoscopy
- Evaluates the lower urinary tract (bladder, urethra) and entrance of ureters
- Can be used to diagnose ectopic ureters and in some circumstances combined with treatment
- Urodynamic studies (e.g. pressure cystometry using pressure catheters) to evaluate the presence of contractions of the urinary bladder wall and to assess the urethral pressure profile/tone along urethral length
- Response to treatment can be considered in cases where sphincter mechanism incompetence is considered likely.
Questionnaire for owners of possibly incontinent dogs
- Where and when is it happening?
- Is the dog awake or asleep when it happens?
- Any changes at home?
- What age did it start happening?
- In terms of the incontinence - do they leak as they walk, i.e. constantly dribble or intermittent? (Consider ectopic ureters)
- Do they only leak when lying down? (Sphincter more likely)
- Does it become worse when they are excited? (Stress/behavioural)
- Do they seem aware of the leakage?
- Are they able to void normally?
- Is it worse immediately after normal voiding?
- Dribbling small volumes after voiding can suggest vaginal pooling of urine
- Is there a normal stream of urine produced (may be tricky for owner to observe)?
- Is the bladder properly emptied after voiding? (normal residual volume is <10 mL or 0.2-0.4mL/kg)
- Is anal tone normal? Any other neurological deficits
- Is any straining seen?
- Does the incontinence persist when they are on antibiotics?
- Have you been able to examine the vulva and ideally vestibule for any conformation issues, e.g. vaginal septa or prepuce/penis/prostate?
- Does urine solely come from vulva/penis i.e. no evidence of urine from rectum-can be seen with urethrorectal fistulas.
- Any PU/PD?
- Any improvement with treatment?
- Urinary continence scoring (1-10) can be performed to provide a more objective measure and monitored after medical/surgical intervention
- 1= leaking when walking, running, playing, sleeping, never urinates a full bladder
- 5= leaking mainly when lying down, minimally when walking or playing, leaks immediately before or after urination
- 7.5 = only leaking when sleeping
- 9= urine noted on fur several times per week
- 10 = no leaking reported at all
Management of urinary incontinence in dogs
Urinary incontinence can be quite devastating for both pets and owners, being a common cause of euthanasia and pet abandonment. There are treatment options available for management of certain causes of urinary incontinence, including for a few anatomic variants and for detrusor instability and urethral sphincter mechanism incompetence.
Ideally, some investigations should be performed before considering treatment (in particular, excluding a urinary tract infection).
Medical treatment for urinary incontinence
Medical treatment can be used for the following conditions:
|
Detrusor muscle instability |
||||
|
Drug |
Type of drug |
Mechanism of action |
Dose |
Side effects |
|
Oxybutynin |
Anticholinergic muscarinic drug |
Relaxes the detrusor muscle |
0.2 mg/kg, PO, sid to bid |
Urinary retention Vomiting Constipation Tachycardia |
|
Propantheline |
Anticholinergic muscarinic drug |
Relaxes the detrusor muscle |
0.2 – 0.5 mg/kg, PO, tid |
Pupillary dilation Decreased gut motility Dry mucous membranes |
|
Imipramine |
Alpha- and beta- adrenergic stimulant |
Relaxes the detrusor muscle and increases urethral tone |
5-15 mg/dog, PO, bid |
Seizures, tremors and hyperexcitability. This medication is also used for separation anxiety and may help patients that urinate in the house when they get excited |
|
Urethral sphincter mechanism incompetence |
||||
|
Drug |
Type of drug |
Mechanism of action |
Dose |
Side effects |
|
Phenylpropanolamine |
Alpha-1 adrenergic agonist |
Increases the smooth urethral muscle tone Clinical response is observed in 75-90% of patients |
1-1.5 mg/kg, PO, q 8-24hrs |
Hypertension (monitor blood pressure, particularly elderly patients) Irritability Poor appetite Male dogs less responsive than female |
|
Oestriol |
Synthetic oestrogen |
Increases the smooth urethral muscle tone Clinical response is observed in 89% of patients |
Initial dose 2mg/dog q 24hrs for 2 weeks then reduce to lowest effective dose eg 0.5 – 1 mg/kg, PO, sid Do not use in cats or in male dogs (causes prostatic metaplasia) |
Mammary gland development Vulvar swelling May attract males and very rarely may induce myelosuppression (important to check haematology 1 month after starting treatment) |
|
Testosterone |
Synthetic testosterone |
Activation of androgen receptors and by conversion to oestradiol activation of certain oestrogen receptors. |
1.0-2.2mg/kg IM q 4-8 weeks |
Male dog only Contraindicated if there is prostatic hyperplasia, carcinoma or mammary carcinoma. Use with caution in patients with significant renal, cardiac or hepatic disease. Can reduce blood glucose thus reducing insulin requirements in diabetic dogs. Use with ACTH or corticosteroids may result in oedema; caution with cardiac and hepatic disease. |
Combination treatment can be used eg phenylpropanolamine and oestriol.
Male incontinence due to USMI is more challenging to treat than in female dogs.
When to consider surgical treatment for urinary incontinence in dogs
Indications:-
- Correction of anatomical variants
- Urethral sphincter mechanism incompetence when medical management has failed or becomes refractory, if side effects develop, or if owners are reluctant to administer long term medication.
- Surgical options are not always effective and might be associated with long term complications, including scar tissue formation and difficulties in passing urine.
Surgical treatment for urinary incontinence
This is a brief overview of surgical treatment options. Surgical treatment can be used to manage certain anatomic variants to correct ectopic ureters, persistent urachus and urethral-vaginal fistulas. For example:
- Laser “cut” technique: intramural ectopic ureters can be cut using a laser beam through urethroscopy
- Surgical techniques for ectopic ureter correction: neoureterostomy, neoureterocystostomy, or nephroureterectomy
Surgical treatment can also be used to manage urethral sphincter mechanism incompetence when medical treatment fails to achieve a good response. Some of these surgical techniques might be used simultaneously (e.g. colposuspension and urethropexy) to improve the success of the treatment of the incontinence. Options include:
- Colposuspension:
- The vagina is anchored to the prepubic tendon on each side so that the bladder neck is relocated to intra-abdominal position. Reported success rate is 53% and up to 70% when combined with urethropexy.
- Transobturator vaginal tape:
- A small incision is made on the wall of the vagina and the permanent tape is introduced via the vagina to sit under the urethra and to hold on the pubic bones.
- Urethropexy:
- The urethra is anchored to the abdominal wall at the level of the cranial pubic brim. This will position the bladder neck more cranially.
- Artificial sphincters:
- These are placed around the urethra, externally, and they increase the urethral resistance
- Urethral submucosal injections:
- Collagen is injected endoscopically in the urethra. This increases the urethral resistance. The duration of the effect is not permanent and is variable amongst individuals.
- Botulinum toxin injection
- Botulinum toxin is injected into the bladder wall in 10 locations and has been associated with positive response in up to 70% dog lasting up to 5 mths.
Stem cell therapy may be an option for urethral dysfunction, more information is needed.
Explore more
Jun 9, 2025 10:58:12 AM
How and When to Perform CT Reconstructions for Veterinary Patients
CT reconstructions are a vital tool in veterinary diagnostics, providing detailed images for...
Read more
Jun 9, 2025 10:58:12 AM
Diagnosis and treatment of Leishmania in dogs
This article details the diagnosis and treatment of canine leishmaniosis in dogs. It covers key...
Read more